A 35-year-old patient receives complex aortic surgery and a renewed chance at life
Case Profile
- Condition
- Stanford Type B aortic dissection
- Patient
- Mr. N
- Age
- 35
- Hospital
- Beijing Fuwai Hospital
- Nationality
- Mongolia
Case Overview
A 35-year-old patient receives complex aortic surgery and a renewed chance at life

Cause & Challenge
Recently, 35-year-old Mr. N underwent one of the most complex procedures in cardiac and vascular surgery at Beijing Fuwai Hospital. The operation addressed a life-threatening aortic condition that had placed him at serious risk.

Why China
Harbor Health connected the patient with appropriate Chinese medical resources, coordinated expert review, hospital access, interpretation, and treatment planning based on the case needs.
Treatment & Benefits
High-risk aortic disease stabilized and treated.
Full Story
Recently, 35-year-old Mr. N underwent one of the most complex procedures in cardiac and vascular surgery at Beijing Fuwai Hospital, addressing a life-threatening aortic condition.
The danger appeared suddenly, turning an undetected aortic disease into an urgent, high-risk situation.
In late 2024, Mr. N suddenly experienced severe chest pain that radiated to his abdomen, a tearing pain accompanied by profuse sweating and fainting. After seeking care at the Third National Hospital in Ulaanbaatar and private hospitals, his family contacted Harbor Health. Harbor Health arranged a remote consultation between Chinese and Mongolian physicians, helped confirm a Stanford Type B aortic dissection, and coordinated blood pressure control, pain management, travel, and admission to Beijing Fuwai Hospital.
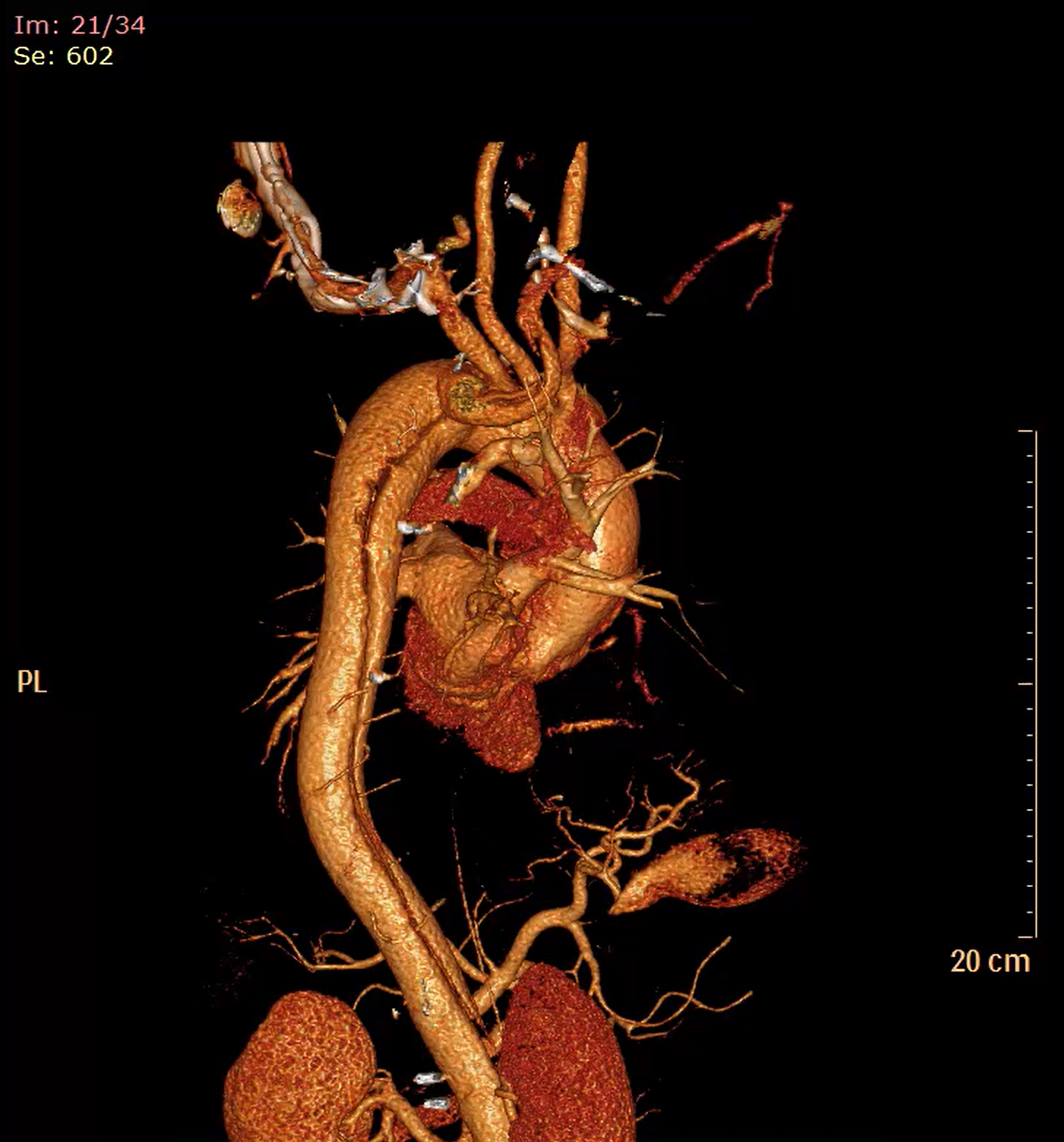
Illustration: Mr. N's Stanford Type B Aortic Dissection disease
After a comprehensive examination, Mr. N's condition was found to be far more complex than initially thought: the aortic dissection was extensive, and he had an aberrant subclavian artery malformation, making conventional surgical methods unsuitable. Given Mr. N's age and the complexity of his anatomy, the specialist team developed a two-stage surgical plan to reduce risk and support his return to daily life. The first stage of surgery, a femoral artery-to-femoral artery bypass graft, yielded immediate results: blood supply to his lower limbs was restored, chest and abdominal pain was significantly reduced, blood pressure was stabilized, and the aortic dissection was stabilized. The first-stage procedure stabilized the immediate risk and prepared him for the second-stage operation.
Pictured: Mr. N after completing the stage 1 surgery.
Multidisciplinary planning for a highly complex operation
Six months after his first surgery, Mr. N returned to Beijing Fuwai Hospital. Professor Yu Cuntao, director of the Vascular Center, led a specialized team, together with Deputy Director Gao Wei, and brought together anesthesia, surgery, extracorporeal circulation, and intensive care specialists to develop a definitive surgical plan for Mr. N.
The team used the "total thoracoabdominal aortic artificial blood vessel replacement" technique, which involves opening both the chest and abdominal cavities simultaneously (through an incision about 1 meter long from the armpit to the abdomen) to perform a total thoracoabdominal aortic replacement, replacing the diseased vessel with an artificial graft, rebuilding blood supply to vital organs, and repairing intercostal arteries that supply the thoracic vertebrae and ribs.
This procedure, total thoracoabdominal aortic replacement with an artificial graft, is widely considered one of the most demanding challenges in cardiac and vascular surgery.
Its complexity comes not only from the length of the operation and the size of the incision, but also from the anatomy involved, the physiologic stress on the body, the level of risk, and the need for coordinated expertise across the medical team.
Why this operation is so complex
1. The scope and scale of the surgery are enormous.
Extensive anatomical scope: The surgery requires replacing the entire aorta from the thoracic cavity to the abdominal cavity, involving both the chest and abdominal cavities and requiring careful management of structures that pass through the diaphragm.
The aorta is interconnected with many organs: it directly branches off to supply all the important blood vessels to the liver, spleen, stomach, intestines, kidneys, and spinal cord. The surgery must interrupt the blood supply to these organs and perform vascular reconstruction, which is equivalent to performing "vascular bypass" on multiple organs simultaneously.
2. Extremely high technical complexity and precision requirements.
Multivascular reconstruction: During the procedure, the blood vessels supplying the abdominal organs (abdominal cavity, superior mesenteric artery, renal artery) and the spinal cord (intercostal arteries, lumbar arteries) must be reanastomosed to new artificial blood vessels sequentially or simultaneously. The anastomosis of each blood vessel requires precision, no leakage, and no torsion, otherwise the affected organ may be placed at serious risk.
Spinal cord protection: This is one of the biggest technical challenges. The blood supply to the spinal cord is extremely fragile, and intraoperative aortic occlusion can easily lead to spinal cord ischemia, resulting in postoperative paraplegia. Therefore, complex auxiliary techniques are required, such as cerebrospinal fluid drainage, staged distal aortic perfusion, hypothermia, and evoked potential monitoring, which greatly increases the complexity of the surgery.
Limited surgical field: the working space is deep and narrow, especially when reconstructing abdominal branch vessels, requiring exceptional precision and stamina from the surgical team.
3. The physiological disturbances are extremely severe.
Risk of massive bleeding: The aorta is the largest artery in the human body and has extremely high pressure. The entire procedure carries the risk of catastrophic bleeding.
Multiple organ ischemia-reperfusion injury: When blood supply to organs such as the liver, intestines, kidneys, and spinal cord is interrupted and then restored, a large amount of toxins and inflammatory mediators are produced, which may trigger systemic inflammatory response syndrome and, in severe cases, lead to multiple organ failure.
Major hemodynamic shifts: when the aorta is clamped and reopened, blood pressure can fluctuate sharply, creating major challenges for anesthesia management.
4. Extremely high risk, serious complications.
Mortality rate: Even in top medical centers, the perioperative mortality rate can still be as high as 5%-15% or even higher, which is much higher than that of routine cardiac surgery.
High incidence of serious complications:
• Paraplegia: The most catastrophic complication, with an incidence rate of approximately 2%-10%;
• Acute renal failure: requires dialysis;
• Respiratory failure: requires long-term mechanical ventilation support;
• Intestinal ischemia and necrosis;
• Massive bleeding;
• Infection.
5. It is a systemic test for the medical team.
"Marathon" surgery: usually takes 6-12 hours or even longer, requiring the surgeon, assistants, anesthesiologist, cardiopulmonary bypass specialist, and nursing team to maintain a high level of focus and physical strength.
Multidisciplinary collaboration: It requires seamless collaboration among top experts from multiple departments, including cardiac and vascular surgery, anesthesiology, extracorporeal circulation, intensive care unit, blood transfusion, neuromonitoring, and nephrology.
Perioperative management is complex: Postoperative patients may require monitoring and treatment in the hospital for several weeks, and the management of every aspect, including respiration, circulation, renal function, coagulation, infection, and nutrition, is crucial.
In practical terms, the procedure requires replacing the body's central arterial channel while maintaining blood supply to multiple vital organs and reconnecting essential branch vessels with precision.
Successfully completing this type of surgery reflects the strength of the cardiac and vascular surgery team, anesthesia, intensive care, nursing, and the broader perioperative system.
An eight-hour surgery with coordinated specialist support
On the day of surgery, Professor Yu Cuntao served as the chief surgeon, with Associate Chief Physician Gao Wei and others working closely together. The anesthesia, extracorporeal circulation, and surgical nursing teams provided full support throughout the procedure.
Illustration: total thoracoabdominal aortic artificial blood vessel replacement
During the surgery, the doctor first cut off the diseased blood vessel, then carefully separated the various branches of the blood vessel, and then used the method of "segmental anastomosis + protection of organ blood supply" to reconstruct the blood vessel: the upper end of the artificial blood vessel was connected to the descending aorta, the blood vessel wall supplying blood to the thoracic vertebrae and ribs was preserved and connected to the artificial blood vessel, and then the blood vessels supplying blood to the stomach and kidneys were anastomosed to the branches of the artificial blood vessel one by one. Finally, the distal end of the artificial blood vessel was connected to the artery at the root of both legs.
The anesthesia team also faced significant challenges: they not only had to precisely control blood pressure and heart rate, but also monitor urine output and intracranial pressure in real time, reduce the risk of spinal cord ischemia by releasing cerebrospinal fluid, and maintain one-lung ventilation to ensure a clear surgical field while preventing the patient from experiencing hypoxia.
The surgery followed the planned sequence, with each stage requiring careful judgment and precise execution. After eight hours, the team completed the procedure successfully.
Recovery milestone: from critical condition to standing again
After the surgery, Mr. N was transferred to the intensive care unit for close monitoring. For him, the successful surgery was only the first step; he still had to overcome several hurdles, including organ damage, awakening, and limb movement.
Pictured: Mr. N, who was discharged from the intensive care unit on the 5th day after surgery.
His recovery progressed well: on the second day after surgery, his endotracheal tube was removed, he was breathing independently, and he could move his limbs normally. On the fifth day, he left the intensive care unit and returned to a regular ward.
Mr. N has now returned to daily life. Looking back on the medical journey, he and his family expressed deep gratitude for the care he received.
Note: This international medical case was compiled from patient or family interviews. Important details and images have been protected to preserve privacy and data security.
For more information about medical travel to China or remote consultations with Chinese specialists, please contact Harbor Health.